Ten Places Where Collective Impact Gets It Wrong April 8, 2016
Posted by tomwolff in : Uncategorized , add a commentThe following was published in the Global Journal of Community Psychology Practice (www.gjcpp.com) in March 2016 .
Summary Table: Ten Places Where Collective Impact Gets It Wrong
Tom Wolff Ph.D
1) Collective Impact does not address the essential requirement for meaningfully engaging those in the community most affected by the issues.
2) A corollary of the above is that Collective Impact emerges from top-down business consulting experience and is thus not a true community development model.
3) Collective Impact does not include policy change and systems change as essential and intentional outcomes of the partnership’s work.
4) Collective Impact as described in Kania and Kramer’s initial article is not based on professional and practitioner literature or the experience of the thousands of coalitions that preceded their 2011 article.
5) Collective Impact misses the social justice core that exists in many coalitions.
6) Collective Impact mislabels their study of a few case examples as “research”.
7) Collective Impact assumes that most coalitions are capable of finding the funds to have a well- funded backbone organization.
8) Collective Impact also misses a key role of the Backbone Organization – building leadership.
9) Community wide, multi-sectoral collaboratives cannot be simplified into CI’s five required conditions.
10) The early available research on Collective Impact is calling into question the contribution that CI is making to coalition effectiveness.
Tom Wolff & Associates,Leverett, MA. tom@tomwolff.com, www.tomwolff.com
http://www.gjcpp.org/en/resource.php?issue=21&resource=200
| Would love your thoughts. | Please share and disseminate. |
The Emerging Non Profit World in Saudi Arabia: A Promising Glimpse January 8, 2015
Posted by tomwolff in : Uncategorized , add a comment

Tom Wolff addressing conference in Khobar, Saudi Arabia

The email arrived out of the blue in June of this year. The email was titled, “Invitation to speak at top Saudi NPO Conference!” They were inviting me to give a keynote address in early November at the annual non-profit conference at King Fahd University of Petroleum and Minerals in Khobar in the Kingdom of Saudi Arabia. I was baffled – how did they find me? Why did they want me? What were they asking of me?
The last question was made clear in their email: “Knowing you are an expert, academic and consultant in the field of community development, we would like to invite you to speak at our conference and give a keynote presentation about community development and the role of the non-profit sector in light of the roles of the other two sectors (public, business).”
So,over the next few weeks and months we talked, emailed and negotiated the topic and content of my talk. Ultimately it was titled: Enhancing Collaboration Across Government, Business and Non Profits: Building Healthy Communities in Saudi Arabia. Throughout that time I wondered what they really wanted from me, what was awaiting me, and what was happening in Saudi Arabia. I let them know that all my community development work and healthy communities work is based on core principles of democracy and was that going to be okay to discuss in the Kingdom of Saudi Arabia (KSA)? They reassured me that it would be fine. So, I proceeded with their support to acquire a visa and booking flights etc.
I read a few books on visiting Saudi Arabia and started to learn about the country as best I could from here in the US. I learned about the ‘religious police’ who enforce the wearing on burkas for women. I watched a wonderful Saudi movie, Wajdja, (from a female director) about a girl wanting to ride a bike (not acceptable). I checked out the websites on “women driving in Saudi Arabia” – which states that this is the only country in the world where women can’t drive. I learned that a large percent of the Saudi work force (especially lower level jobs) were performed by foreigners (ie 1.5 million from the Philippines). I read on the visa application that violations of Saudi drug laws were punishable by death. I was fascinated and remained baffled.
I was told that there are 1400 non-profits in Saudi Arabia, 700 of them being Islamic teaching organizations. That leaves 700 doing the work that non-religious non-profits do here in the US. That’s not many non-profits, I imagine we have 700 non-profits just here in western Massachusetts.
They later informed me that on top of the keynote they also wanted me to offer a 6 hour workshop on the actual ‘how to’s’ of community development and to consult on some of their projects while I was there — it was going to be a busy visit.
Just before leaving, I learned of the amazing roster of presenters that they had lined up for this two day event: Bunker Roy and Meagan Carnahan of the Barefoot College in India; Iqbal Quadir from MIT focused on inclusive ventures in low income countries ie. Grameenphone in Bangaladesh; Aaron Hurst on the Purpose Economy and Pro Bono as a Powerful Solution; Rodrigo Baggio of Brazil Center for Schools on Digital Inclusion in Rio’s favelas; Tony Meloto who builds sustainable communities in slum areas in the Philippines, Farm Village Universities; Robert Ashcroft from Arizona State University on Creating and Sustaining Non -profit Workforce; Michael Grogan from Calgary, Canada on Workforce development in non-profit sector;, and Stephen Brien from England on Social Impact Bonds. This was a much more fascinating line up of speakers than I have heard at a US non-profit conference in decades.
Most of them were much more prominent on the global scene than I was ie. Bunker Roy one of “ the 100 most influential people in the world” and Rodrigio “top leader in South American to watch” both by Time Magazine. But as my visit evolved it became clear that my host, Salem Aldini (a professor of mechanical engineering), was planning to develop a Non Profit Institute at King Fahd University and to launch community development projects across the country starting with a few pilots. This was my area of expertise.
So I began to understand that I was chosen as someone who could convey specific processes and tools for their hand- picked audience of 150 non- profit and family foundation leaders. I could also expose them to tools in the Community Tool Box (ctb.ku.edu) which is translated into Arabic.
During my four days I began on day one by working with a small group consultation with the faculty who would be the facilitators in my upcoming six hour workshop, gave the kick off keynote address, followed by an afternoon discussion session. Then, two days later, a consultation to the teams planning the community development pilot and another team working on youth interventions who were looking for innovative ways of assessing youth needs. Finally I delivered a six hour workshop to a small hand chosen group of 35 non- profit and foundation leaders. It was a workout for them and me.
The Saudi faculty, foundation and non- profit leaders whom I met with in the small group consultations were very serious about trying to bring community development innovations to the Saudi non- profit and foundation world. They asked lots of questions, took lots of notes. Clearly , they were most curious about this work. This is startling in light of the repression and limited practice of democracy in Saudi Arabia. We often got to the point in a discussion, especially when talking about evaluation and documentation, where they said that although the government collects data it is generally unavailable to those in the university , foundation and the non-profit world.
In one small group I did learn of people working at the community level bringing the three sectors (business, government, non- profit) together to address crises over the last few years such as: the flooding in Jeddah, the influx of Kuwaiti refugees after the Gulf War, and helping female teachers get transportation to work.
The second class citizenship of women was always present in our discussion. The keynote audience was all male in the auditorium, while the talk and slides were also shown in a separate conference room to the women. At the buffet breakfast one morning a woman in full burka addresses me; she was a participant in the other room – liked my talk but complained about Bunker’s Barefoot College because it took the Grandmas away from villages to become solar engineers. Why not take the men? She is Secretary General of the International Islamic Women’s Association. I asked if it was alright for me to sit with her for breakfast (I was fascinated). Although, she said ‘yes’, when I sat down she spent all her time of the cell phone – so I assumed it was not really acceptable and I moved.
A few people attending the conference explained to me that Mohammed both worked and prayed side by side with his wife – so that the precedent for the separation of the women was not really clear.
Of course, in most cultures, to my knowledge women do the core community building work , often below the radar. That has been true in almost all my community development and coalition building work in the US. But in KSA, it is tricky to build coalitions because men and women have to be separate – we were deep into a conversation about a planned model community development project in a limited geographic area (a city neighborhood) when I asked whether we would be able to mobilize the men and the women together – I was told “no”, that it would be two separate but coordinated efforts – mind boggling to an American community builder.
But interestingly enough, at 9 PM in my workshop all of a sudden a number of the men left – I was later told that they had promised their wives that they would be home by 9 PM!
Religious questions often surfaced during my visit. In almost all the question and answer sessions there would be statements about what the Koran said. Often these questions were not really questions but some statement of Islamic teachings that might or might not relate directly to what had just been said. Many of the Saudis were eager for us to leave with a better understanding of Islam. To that end, we were presented with copies of the Koran and a six set DVD set on understanding Islam.
My workshop was entitled “Enhancing Collaboration with Government Business and Non Profits – A workshop on Tools and Processes for Success.” It included an overview of collaboration, and the five key principles of collaborative solutions from my book (The Power of Collaborative Solutions). I helped them take a view of non-profit functions beyond individual, remedial work done by professionals and to expand to working with families, tribes, the whole society and going beyond remediation to include prevention, development and empowerment as legitimate non-profit functions. This seemed to be an important expansion of scope for them. We covered planning tools such as: coalition start up and planning, SWOT Analysis, visioning, force field analysis, developing a road map, barriers, tools for engaging the community and finally collaborative leadership. The Community Tool Box was demonstrated. The participants were eager to engage with all the material but it was hard to tell exactly how much they would actually take back with them and use. Doing an English/Arabic bilingual workshop for 35 participants over six hours with two breaks for prayer was a new experience for me. Having all the worksheets translated into Arabic was wonderful but it made it impossible for me to indicate which was the appropriate page. They all seemed to humor me as we proceeded, and I will be anxious to see the evaluations. The informal feedback after the workshop was very positive.
Some startling other learnings:
- English is the official language at King Fahd University (and also in the Saudi business world), KSA was described jokingly as the 51st US state.
- The average size of a Saudi Family Foundations was said to be $10 Billion!
- The warmth and hospitality of the Saudis was remarkable. People were always offering to help and sincerely interested in our well- being during the stay. One afternoon my very accommodating host, Ahmad, was going to take me to a store where we could buy dates to take back to my family. We went to the nearby mall but it was closed for prayer, so as we were leaving we saw two men having a cup of coffee (or Arabic tea). Ahmad asked them for a recommendation of a store and directions and they had a lengthy chat. We then went to find Ahmad’s car, but just like in the US who can find their car in a Mall’s parking lots? About five minutes later one of the men we had just talked to came running up. He had thought of a better date store for us to go to. Amazing hospitality!
So what did I bring home?
I loved the adventure and foreignness of the whole experience in a totally different culture.
I was excited by the opportunities that Salem Aldini has opened up for a developing non-profit world in KSA
I am eager to help in the next phases of their progress. Many participants indicated that they were eager to have me come back – but in all honesty I am not sure that that wasn’t just Arabian hospitality and warmth. On the other hand, Salem informed me that he arranged for my visa to be good for five years (the visa is in Arabic so I have no idea what it says) – so maybe I will return. I would enjoy that.
Also, I was able to reflect on how my enthusiasm for the future of non-profits in KSA did not match my experience of the non- profit world in the US in 2014. Here, I see the non- profit world becoming increasing conservative, become averse to risk, and to sticking their neck out and naming the issues that stare us in the face (racism, economic inequality, etc.). Maybe we in the US can re-capture that sense of adventure that comes from an emerging non-profit sector – but I am not sure what will make that happen.
Tom Wolff
December 2014
Add a comment
Tapping our passion for addressing systemic racism and social justice: Keeping your coalitions going after your grant money runs out October 29, 2013
Posted by tomwolff in : Uncategorized , 2commentsOver my forty years in the nonprofit world I have seen many multi-site coalition efforts come and go. They rise and fall with the funding whims/fads of government whether it is substance abuse, violence prevention, teen pregnancy prevention etc. I’ve never seen one of these multi- site networks of coalitions sustain themselves without either new funding or the support of the original lead organization.
The New England Racial Justice and Health Equity is the exception, so it is story worth telling.
The original network of Health Equity and Racial Justice coalitions was created by CDC REACH (Racial and Ethnic Approaches to Community Health) grants awarded to the Boston Public Health Commission’s Center for Health Equity and Racial Justice. The BPHC Center funded efforts at 13 sites across New England from Manchester NH to Springfield MA and Bridgeport Ct and obviously in the Boston area as well. I was a consultant/trainer to the Center and many of the New England sites over the five years of funding.(See below for references to the Center’s work and to my writing about their work).
The core approach of addressing health equity was through a model (see chart) that acknowledges the critical role of systemic racism in health outcomes.
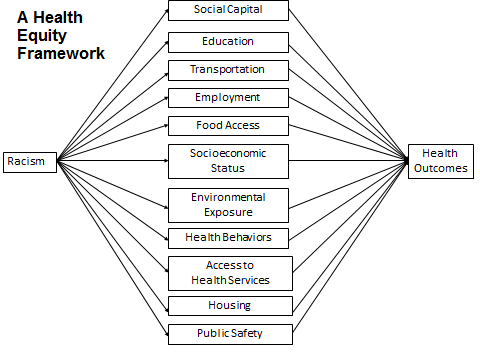
The goals of the coalitions were to create policy changes to address systemic racism in the social determinants of health (exs. food access, educational disparities).
The issue of racism was central to these efforts from the start. For example the first BPHC brochure focused on breast and cervical cancer in Black women. The brochure language was explicit: “If you are a Black woman living in Boston and you have a greater chance of dying from breast or cervical cancer than a White woman. Why? Racism may play a key role in determining your health status. It may affect your access to health services, the kind of treatment you get and how much stress your body endures.”
Based on this health equity framework each team at all 13 sites went thru anti-racism training and learned to re-frame their community health issues in racial justice /health equity terms. This led to struggles to come to grips with racism in both their community and in themselves regardless of their racial and ethnic identity. Over time each community faced significant ‘push back” from some forces in the community to the explicit focus on and use of the term ‘racism’. In fact, most efforts to address health disparities in the U.S. avoid explicitly using this term and instead create programs that ‘blame the victim’ i.e address health disparities in diabetes in Black men by running programs for Black men on eating well.
By acknowledging that racism is the core issue in health disparities we stirred the social justice roots of the staff and communities at the sites. This was powerful enough to keep the discussion going after the money ran out. At the last meeting before the funding ran out in October 2012 the leaders and staff from many communities expressed the desire to keep meeting. The CDC no longer was providing money, and the BPHC being a city health department could not take responsibility for organizing a New England wide group; but the group was determined. There was a strong desire to keep the discussion of race and the struggle for social justice alive.
So we named ourselves the New England Racial Justice and Health Equity Coalition and have kept meeting quarterly on a purely voluntary basis. One site acts as host for each meeting and designs the meeting, and provides the food. Sometimes if the site is short of resources we pass the hat to cover food costs.
At the first meeting we did ‘push back circles” a process designed by one site to allow the group to role play real examples where they experienced difficult ‘push back’ around racism from their community. However, this time in the role play they have three coaches to help them with feeling supported, finding the language to respond, and managing their emotions. Everyone found the experience very helpful and brought their learning back to their communities.
This process of quarterly meetings has now lasted for a full year. Part of each meeting is now spent in ‘affinity’ groups with the White participants, and communities of Color meeting separately for part of the meeting. This allows for a different level of discussion on race than usually occurs in mixed groups. As a White man I have certainly found this approach allows me to explore how I can use my White privilege to best advantage in moving this work forward without making things worse.(see the work of Tim Wise as an outstanding example of understanding white privilege (http://www.timwise.org).
I have learned many things in the process of this experience. The lesson around sustainability seems to be that when we tap into people’s strong passions for social justice we are able to keep many people at the table even when the money has disappeared. Thus, we have another great reason to keep issues of social justice high on our agenda.
After the Trayvon Martin trial there was a national outcry for discussions of race in America. Is there a place for in your community for those discussions? And for tackling the work on health equity and racial justice through a transformative change lens?
References:
The Center for Health Equity and Social Justice’s work has been published and is available at (http://www.bphc.org/chesj/Pages/default.aspx)
I have also written about this work (https://www.tomwolff.com/collaborative-solutions-newsletter-summer-10.htm), and have had articles and videos published in the Global Journal of Community Psychology Practice See below:
What else is new at Tom Wolff and Associates?
New Publication:
“A Community Psychologist’s involvement in policy change at the community level: Three stories from a practitioner” by Tom Wolff, PhD, Amherst MA, USA.
In the Global Journal of Community Psychology Practice: Peer reviewed http://www.gjcpp.org/en/article.php?issue=14&article=68
“As a community psychology practitioner who works with local communities policy change has always been an integral part of my work. This paper will illustrate that influencing social policy for community psychologists working in communities is a natural part of their everyday activities. Every dilemma faced by communities not only has programmatic solutions but also root structural causes that require policy changes. Often our task is to build the capacity of the community to become effectively involved with local office holders on issues of policy change.”
A familiar resource in a brand new package: The Community Tool Box http://ctb.ku.edu
I have been a member of the Community Tool Box team for the twenty years of its existence. We are very excited to announce a new look for the tools you love!
The Community Tool Box team just launched a new site, full of tools to change our world. If you’re not yet familiar with the Tool Box, it contains over 7,000 pages of practical information for skills such as those related to community assessment, strategic planning, intervention, evaluation, advocacy, and sustainability. The Tool Box is now used by over 4.4 million unique users from 230 countries worldwide, and builds the skills of professionals and local leaders working collaboratively to improve socially-important issues.
Exciting updates to the Tool Box include:
- Responsive design: fits mobile devices and tablets
- Easier navigation
- Resources available in English, Spanish, and now Arabic
Old user or new just check out the new look: http://ctb.ku.edu
Some recent clients at Tom Wolff & Associates:
Connect 2 Protect, HIV Prevention, Fenway Institute Ongoing Consultation 2013
Metrowest Health Foundation, Leadership Training, Framingham , MA. March 2013
Kansas Health Foundation, Recognition Grant Conference, Coalition Building Training, March 2013
Oklahoma State Health Department. Public Health Leadership Institute ,June 2013
Healthy Wisconsin Leadership Institute, Training on Sustainability, June 2013
Family Crisis Center of East Texas, Day long retreat, Nacogdoches TX. August 2013
2commentsWhere oh where have all the grassroots gone? May 30, 2013
Posted by tomwolff in : Uncategorized , add a commentIn my trainings on coalition building and community development to non-profit human service and health providing organizations I always emphasize the importance of engaging those most affected by the issue – sometimes called the grassroots communities. Depending on the focus of the work this can mean: youth, immigrants, communities of color, survivors of domestic violence, the LGBT community, etc. We cannot do authentic community work without their voices at the table as shared decision makers. In my experience when we do not have them at the table we develop programs that are more likely to be ineffective.
At the start of my trainings I often explore this issue using an experiential tool called ‘Stand and Declare’. I place a statement on the screen and ask participants to go to one of five stations around the room that are marked strongly agree, agree, neutral, disagree, and strongly disagree. They then talk about why they chose that position. One statement I have used in this exercise for almost a decade is “In our community work we always engage those most affected by the issue and they willingly come to the table and participate actively”.
Working with these non- profit providers over the years I have always received more ‘disagree’ than ‘agree’ statements. The grassroots approach has never been the way that the mainstream of health and human services have functioned in the last decades. However, recently in the group discussions that follow I have seen a very disturbing trend. Increasingly there are fewer and fewer people who not only disagree but who do not actually even try to engage the grassroots anymore. Although most folks seem to still agree that we “should” do this, in fact very few even try to engage the most affected community.
This is very disturbing for those of us who believe that this is the basic building block of any authentic community building effort in the non-profit, health sectors and beyond. How can we design programs for communities without having them at the table?
One advocate for this grassroots approach is Barbara Ferrer, the Commissioner of Public Health for the City of Boston. She puts it this way: “The role of a public health department is to create a space for residents to come together to define a problem, to define the solutions, and then enter into a dialogue with us—not the other way around. Not we define the problem, we define the solution, and then we invite you in to help us implement the solution, which is what we’re most comfortable doing.”
The ones who succeed at this tell us consistently that there are a series of efforts that we must make to adapt our practices so that the community can come to the table. These include: holding the meeting in the evenings, providing child care and transportation, feeding the group, providing translation services if needed, and even providing a stipend (a coupon for a local grocery store etc.).
So what is happening? Why don’t we seemingly do this anymore?
– Maybe we don’t want to share power and no one is pressuring us to do it.
– Or is it that government and foundation funders seem to demand this kind of involvement less often ( in the past it was the serious demands from funders that often drove the nonprofits to bring the grassroots to the table). In one state the Sexual Assault Prevention Coalition coordinator told me that her Rape Prevention Education Grant to the CDC was turned back to her because she used the phrase “grassroots”. She was told to remove the word if she wished funding.
– Could it be that the adaptations above (transportation, baby sitters, etc.) are too much to provide? So it becomes more difficult than the nonprofit world wants?
– Or is it the arrogance of the helping world is growing during tighter financial times, especially as we have more large mega-agencies and fewer small community non-profits
– Maybe we settle for the usual suspects who are the gatekeepers (i.e. the easy to reach minister) rather than do the hard work of identifying and recruiting the grassroots community.
I know very well that a small handful of people in the non-profit human service and health world are doing terrific work at still engaging the grassroots community and we should identify and celebrate those efforts (maybe on these pages)
On the other hand if you also have seen this negative trend what is your guess as to why it is happening?
And what can we do about it? What have you observed?
Tom Wolff, Tom Wolff & Associates, Amherst, Massachusetts May 2013
Add a commentPost election Collaborative Solutions Newsletter issue November 10, 2012
Posted by tomwolff in : Collaborative Solutions , add a commentDear Friends and Colleagues,
The Newsletter is Back!
And what timing……. the pundits have said it ‘ post-election America is in dire need of collaborative solutions’. So we all move forward in our work to build a ‘commons’ where we can address our differences and build exceptional healthy communities.
The Fall 2012 Issue of the “Collaborative Solutions Newsletter” from Tom Wolff & Associates is on “Managing Multiple Coalitions: Mission Possible”. In the newsletter I offer seven keys to successfully managing multiple coalitions.
This newsletter issue and earlier issues are available online at www.tomwolff.com. You may find that the web versions to be the easiest to read and download. A text version can be found below.
We encourage you to distribute this information. Please feel free to download this issue at www.tomwolff.com and circulate it to your friends and colleagues. You can subscribe for free at the end of the newsletter online. Let us know what you think and what else you would like to see in the newsletter.
Thanks
Tom Wolff
Tom Wolff & Associates
In this issue:
For Those Managing Multiple Coalitions: Mission Possible
The seven keys to success
- Site selection
- Orientation and ongoing training for teams
- Building a larger learning community
- Paying attention to leadership and membership
- Managing conflict
- Strategic planning and action
- Monitoring and creating systems of accountability
What is new at Tom Wolff & Associates
For Those Managing Multiple Coalitions: Mission Possible
In both public and private spheres, many foundations and agencies create and fund systems of independent coalitions working at various geographical sites on the same issue. For example, a state health department may wish to encourage the creation of local food and fitness coalitions. So the department issues an RfP and chooses twenty coalition applicants from across the state to be funded to implement the project. This is how big ideas can be spread across a state, a region, or even an entire nation.
As the people involved in setting up and managing multiple coalitions at many sites often discover this can quickly become a logistical and organizational nightmare
Over the last thirty years, I have frequently been asked to design, train, and consult with these kinds of multiple coalition systems. While the complexities can be challenging, the successful outcomes have been exhilarating for everyone involved.
A common “wisdom” of coalition success is the “Law of Thirds”: if you set up coalitions in every state in the country or every county in your state, one third will succeed, one third will struggle but make progress, and one third will fail. In fact, coalition outcomes often look like this. However, no one ever sets up their system of coalitions with such limited hopes. At the outset we all seek 100% success. So how do we surmount the common wisdom and achieve extraordinary results?
The consulting work I have done for numerous multiple-site coalition systems has helped people combine their forces to solve problems relating to an extremely broad range of topics. Here are a few examples of multiple-coalition systems that have asked me to facilitate their multifaceted efforts:
- The National Funding Collaborative on Violence Prevention (now the Institute for Community Peace) works with coalitions across the United States on a variety of forms of violence prevention and peace promotion.
- Healthy Communities Massachusetts was initiated by our own nonprofit, Community Partners, to build healthy community teams in cities and towns across Massachusetts.
- The Boston Public Health Commission’s Center for Health Equity and Social Justice’s REACH 2010 health-equity grant sites learned to work together through consultation and training.
- The Healthy Wisconsin Leadership Institute brings me in annually as a trainer and consultant to statewide teams.
- The Centers for Medicare and Medicaid Services End-Stage Renal Disease Networks brought me in for training and consultation, and over a few years we built the organizations’ capacity to develop regional coalitions on a number of critical topics, like disaster planning.
These are examples of multi-site coalition systems that have succeeded. As we have done this work universal dilemmas, lessons and tools have emerged that can be helpful for those designing and managing systems of multiple coalitions. These coalitions have succeeded by paying attention to seven key areas; these areas can make the difference between success and failure for multiple-site collaborations:
- Site selection
- Orientation and ongoing training for teams
- Building a larger learning community
- Paying attention to leadership and membership
- Managing conflict
- Strategic planning and action
- Monitoring and creating systems of accountability
Let’s look at the seven keys to success in more detail.
1. Selecting sites
Site selection generally occurs through an application process, the administrative body issues an RfP and asks coalitions/communities to express their interest in participating and to make a case for their group’s inclusion. This can give us more information for selection, but even when we carefully evaluate applicants all we can do is make our best guess about which groups will work well together, or even put out effort toward the goals. Little data seems to exist to predict how to choose good performing coalitions.
In evaluating applicants it is good to look for:
- A sense that the group understands the goals of the coalition.
- Some excitement from the group about engaging in the venture (just the fact that they have applied show some interest).
- Some competence within the applicant group in the content of the coalition work (i.e. food and fitness)
- A track record of getting results through coalition building.
- Lastly, a clear proposed plan to proceed.
Yet when we look back at the selected coalitions that later failed, the hints that would have let us predict the failure were not always evident in the applications. In one recent example, an applying coalition looked really competent in their application, but only wanted to get access to more money to promote its existing agenda and had no interest in the extra work that we were supporting. This self-serving purpose only became obvious after we had funded them.
2. Providing orientation
At the start of an initiative, orientation of new sites is critical. I have seen many variations of how orientation can be carried out.
Orientation is the time when the funder shares very clear expectations about what is expected from the participating coalitions. This is tricky. We often create coalitions because we want to create broad changes that require community input. By definition, our ideas have a large scope. The trick comes in allowing for this large scope and for community ownership and creativity, while still being clear about the specific outcomes that we intend to achieve.
We learned this the hard way, in the early years when our vision and optimism ran high and we had far less experience to let us look to the future and predict, and prevent problems. When we initially launched Healthy Communities Massachusetts in the early 1990s, the field was young and we were naïve, enthusiastic, and grandiose. So we left the specific goals vague, in terms of both content and process, in the hope of encouraging the participants’ creativity and ownership. We paid a price with the resulting chaos. In future rounds, we got better at setting expectations while encouraging community input—and our outcomes improved dramatically.
As we consult with other groups now, we see projects that err in both directions either by asking too much or too little of the collaborators at the start. From the obvious risks of “too little,” some funding authorities have moved toward “too much”. I now work with some groups where the funder dictates everything, down to the number of minutes committed to a meeting’s agenda items.
In many contemporary public health projects, we want to look at changing specific indicators in the context of the social determinants of health (SDOH). This is a very broad scope. So when we orient a group to achieve a goal like this, what specific objectives do we want to outline for them? If the coalitions feel they need to accomplish something concrete, they will focus on the indicator and ignore the social determinants. On the other hand, if they concentrate on a broad SDOH community assessment, they may find it hard to show concrete results.
Delicate balances like these can be resolved, but they require careful consideration before the initial orientation takes place.
3. Building a larger learning community
Building a learning community among the participating sites can be one of the most powerful tools for creating a network of successful coalitions. We often ignore the power of peer learning, and as a result we miss great opportunities.
It’s easier to build a larger learning community if you have time on your side. In some situations, we have had grants that have extended over two or three years. Sites had the opportunity to meet at gatherings, including annual trainings, where they could build relationships with each other and share their work. While we began with an expert/training model in early meetings, once some foundations had been established and work was underway it became apparent that the best learning was actually going to happen through the sites’ shared successes and struggles. That sharing had been part of the earliest trainings, but as the project evolved we were able to systematically focus on it. We designed whole meetings, led by team members, in which teams presented their experiences to each other and were paired up to coach each other.
4. Paying attention to leadership and ongoing training for leaders
Let’s consider leaders—both where they come from and what they do. We usually assume that coalitions will be facilitated by people well versed in the world of collaboration and organizational change. We envision these as folks who have been trained in community public health, community psychology, or community development. In fact, few people, even in these fields, have been trained to facilitate coalitions. As a result, coalition leaders come from varied backgrounds and what they have in common is interest and enthusiasm, not necessarily the skills. Thus, it is vital to provide training on many core coalition skills.
I recently trained two sets of coalition leaders at national meetings. The first group was developing statewide breast-feeding coalitions. This passionate group of women is committed to supporting policy change to encourage breast feeding. Most were lactation nurses who had, through a process of evolution, ended up as statewide coalition leaders. The second group consisted of IRS staff (yes, the Internal Revenue Service!) who work in a program that creates local collaborations to help low-income residents get free tax-form help (VITA program Volunteer Income Tax Assistance). These were mostly accountants by training with long histories of doing compliance work for the IRS. They had little to no experience at all with coalition work before they started. Yet, both sets of people were engaged in facilitating coalitions and were eager learners.
There’s no way to tell in advance whether your current coalition leadership is capable of delivering your desired results. No matter who you’re working with, you usually need a comprehensive leadership-training plan. There are lots of ways to accomplish this. For Healthy Communities Massachusetts, we held an annual three-day retreat for our community teams. In these three days, we covered the essentials: coalition building, grassroots community engagement, healthy communities, leadership, racial equity, and evaluation. We followed this up with shorter workshops throughout the year.
5. Preparing to manage conflict
Conflict is inevitable. One question to ask is whether you have adequate mechanisms for managing it.
Many individual coalitions get bogged down in poor facilitation and group processes. In fact, I have met many coalitions that do not even meet regularly! They fail to communicate, and are not clear on roles and responsibilities and decision-making processes. The literature indicates that one of the keys to getting these coalitions to be effective depends on identifying and managing conflict.
Once I was training coalition leaders in northern Minnesota and the discussion turned to the management of conflict. The group informed me that the norm in their area was to be “Minnesota nice,” so that addressing conflict would be a challenge. This is a cultural issue that reaches far beyond northern Minnesota, although the Minnesotans were kind enough to point it out. In truth, conflict-avoidance is often the norm in nonprofit coalitions, no matter where they are located.
For many groups, I suggest a very simple process that will help them address their internal “sticky” situations without frightening anyone. Start each meeting by creating ground rules, or by reviewing existing ground rules. Post these agreed-upon guidelines. An example would be “one person talks at a time.” Another, if there’s a particular member who talks too much, could be to suggest a limit placed any individual’s talking time on a single topic. At the end of each meeting, conclude by making a two column “plus/delta” list, looking for what worked about the meeting (the “plus” items) and what could have been different (the “delta,” or change, items). List the two categories on a newsprint sheet and have everyone contribute observations. In this way you can check as to whether you have respected your own guidelines. These two steps can help identify and address ongoing process issues.
6. Strategic planning and action
Here are some of key questions to ask regarding planning and action:
- Does the project have a vision that the participants have generated together?
More than once I have done training for a coalition that is 6 to 9 months old and has yet to develop a vision. Very easy visioning exercises can prevent this flailing about; see The Power of Collaborative Solutions p.157).
- Are the actions tied to the vision and the goals?
Logic models were developed to guarantee that a link exists between vision/goals and action, but the formal language of “logic model” can be scary for community groups. To get past this barrier see the Tearless Logic Model (http://www.gjcpp.org/en/index.php?issue=7)
- Is your organization converting its ideas into action or does it get stuck in the planning stage?
Many processes involving multiple coalitions begin with lengthy data-gathering phases and/or organizational structure demands (bylaws, 501(c)(3) requirements, incorporation, and so on). This can distract the people in the systems so much that they forget that they have to move to actual community actions in order to create community change.
- Most importantly, do outcomes matter?
The funding organization must make it clear that the whole purpose of these efforts is to create community change and that outcomes really do matter.
- Finally, are the project participants planning for sustainability?
There’s no point in doing the work only to have it fall apart just as it should be generating its own momentum. I have developed a four-pronged sustainability process that needs to be part of the project’s thinking right from the start. It involves finding resources, developing policies, creating community ownership, and institutionalization. http://www.gjcpp.org/en/index.php?issue=1. It’s a lot easier to build this in at the beginning than to realize, as you near the end of the road, that you are about to run out of pavement.
7. Monitoring and creating systems of accountability
Once we have created these multiple-site coalition systems how do we monitor their progress? What process and outcome measures do we look at to determine whether they’re accomplishing what we have asked them to? How do we build in encouragement for those coalitions that are working to create community change, and consequences for less productive performances?
Often we start with process measures: How often are the participants meeting? How many people attend, and who are they? Are there any members of the affected groups? Are the collaborators creating work groups to get the actual tasks done?
It’s more difficult to examine outcomes than processes, because many of these are long term. The work of Fawcett and colleagues suggests tracking and documenting the creation of community changes, which they defined as changes in programs, policies, and practices that will help people reach the desired long-term outcomes (see the Appendix in The Power of Collaborative Solutions). This can help you track progress. But in truth most coalition systems don’t use such specific criteria.
In the meantime, with informal monitoring going on but without clear evidence that their money is being well invested, program administrators have to decide which programs are progressing at an adequate rate; which need to be put on “probation”; and which to drop from their funding list. Sometimes, because measurement seems so hard, these decisions just get finessed and programs that are not performing continue to be funded and supported.
It would be helpful if the formal evaluation processes set up for these systems of coalitions could assess their effectiveness in ways that help funders base their decisions. Unfortunately, program evaluation is often contracted out to a third party and produces data that may be of little value for administrators deciding whether to continue supporting a coalition, or, worse, arrive so late that they are useless.
There are alternatives. Both accountability and performance measures can be built into the operation of the system from the start. Doing this is easier and more accurate than trying to work on these tasks retroactively, and has the strong added benefit of giving the participants ongoing feedback about the effectiveness of their work, which can strengthen their commitment and multiply the positive results of the entire project.
Mission possible: Tom Wolff & Associates can help your multiple-coalition effort.
Whew that’s a lot to keep track of! Designing and implementing a system of coalitions, at any scale, poses many questions. The good news is that technical assistance is available to help you prevent, or resolve, a wide range of problems that may impede the work of your multiple-coalition system.
Whether your responsibilities are focused across a state, a region, or a nation, Tom Wolff & Associates can help you design and sustain a coalition system of excellence that operates efficiently, remains on track, and achieves your desired goals.
Whether you’re just getting going or you’ve reached a point where you’re stuck, contact us at tom@tomwolff.com. It’s easier and more economical to set your system up for success than it is to watch your dreams fade. We can help you work together and achieve the results you envision.
What is new at Tom Wolff & Associates?
New clients at Tom Wolff & Associates:
Internal Revenue Service – Training for leaders covering the whole nation in VITA program IRS in the SPEC (Stakeholders, Partnerships, Education and Communication) division. August 2012
United States Breast Feeding Coalition (USBC) – Training for state leaders from all fifty states with an emphasis on concrete tools to take back home. August 2012
Western University of Health Sciences, College of Graduate Nursing. Keynote training for their conference on Quality and Safety Education for Nurse Educators and Clinical Leaders. Focus on how to build collaboration in increasing safety and quality in hospital care. August 2012.
Family Crisis Center of East Texas, Angelina County SAVE Coalition, Lufkin Texas: Day long retreat to launch sexual assault prevention coalition for the county. August 2012
Massachusetts Home Visiting Initiative – training for leaders from 17 statewide coalitions on early childhood intervention sponsored by the Massachusetts Dept. of Public Health with federal money from the new Health Care Bill. October 2012
Oklahoma State Health Department. Tobacco Settlement Endowment Trust Keynote workshop on Building Health Communities through Collaborative Solutions at statewide annual meeting. October 2012
The Power of Collaborative Solutions
The Power of Collaborative Solutions continues to do well, being adopted by more and more universities for course use. The book also was heavily referenced in Meredith Minkler’s wonderful third edition of “Community Organizing and Community Building for Health and Welfare”
Add a commentSocial Determinants of Health and Mental Health: Why Not? May 24, 2012
Posted by tomwolff in : Coalition Building, Collaborative Solutions , 1 comment so farThe concept of Social Determinants of Health (SDOH) is widely used and accepted as a way of understanding health, especially in the world of Public Health. Social Determinants of Health are the “conditions and environments in which people are born, grow, live, eat work and age as well as their access to the care system” (CDC). The premise behind Social Determinants of Health is that our health is determined by much more than our access to health care and our health behaviors but also by the powerful forces in our environment such as:
- Socio economic status
- Environmental exposure
- Education
- Employment
- Housing
- Access to food,
- Transportation
- Social capital, and
- Public safety.
Social Determinants of Health account for almost 80% of our health. Access to health care actually only accounts for around 10% of our health. There is solid research to back up the impact on health in each of these arenas. The punch line is that our zip code may be more important than our genetic code for our health. A social determinants of health approach allows for a broad, ecological, community wide, understanding of our health and an equally broad approach to interventions to modify these numerous systems to improve health.
So, the question for this Newsletter is, “ why isn’t this simple common sense framework being applied as broadly to mental health as it is to physical health?” There was a conference at the Adler School of Professional Psychology in 2010 that was focused on this topic.(See The Social Determinants of Mental Health: From Awareness to Action June 3-4, 2010 http://www.amazon.com/The-Social-Determinants-Mental-Health/dp/1456324160). But, short of this, the literature on this topic is minimal. This is puzzling since on the face of it mental health seems even more amenable to a SDOH understanding than physical health.
One of the first things I learned in Psychology 101 was that behavior is a function of the organism and the environment. However, as I proceeded in my undergraduate and graduate training, the focus was more and more on the person/organism side of the equation and less on the environment. In spite of this, in my early work as a psychotherapist on a university campus the link was actually quite obvious. Life stresses had an impact on the well being of my clients. The Viet Nam veterans returning to college brought their war experiences to the campus (in the form of what would later be labeled Post Tramautic Stress Disorders). Mothers of young children living in graduate student housing found managing their lives and their children with very little money to be quite stressful. In these cases we went beyond providing psychotherapy but to building community prevention programs for these groups and modifying their physical environment (i.e. building a playground for the children in the married student housing).
After I left the campus, I worked in Consultation, Education and Prevention in a Community Mental Health Center (CMHC) -remember them?. Here again the approach was a SDOH approach (even though we did not know the language then). For me it was an approach deeply embedded in my training and experience as a community psychologist with a premise that behaviors needed to be understood in their context and the eco-system of the individuals. The community psychology approach empowers populations to solve their own problems. Community psychology is committed to developing prevention approaches that include structural and systems change
With all this background in the community mental health movement in the 60s and 70s, you would think that the field of mental health would have been ripe for embracing and championing the SDOH approach to mental health that is the present hot trend in public health. But no!
Along the way, something interesting and distressing happened. Mental health issues became the business of mental illness, and mental illness became conceptualized as a biological illness cured by powerful and profitable medications. A SDOH approach to mental health and mental illness is a direct threat to the model that declares mental illness a biological disorder cured by drugs.
I can hear the echo of one of my mentor’s, George Albee’s words, predicting the biologization of mental health. First, President Reagan turned the national community mental health system that was federally funded into state mental health block grants. What the states knew about was dealing with the chronically mentally ill, so there was no place for prevention, consultation and education in the mental health system and those services disappeared very rapidly under block grants. That is the equivalent of a comprehensive health system eliminating public health. Then, the National Institute of Mental Health shifted from support of CMHCs to funding for research on the biological origins of mental illness. At that point the drug companies moved in and supported these efforts. The Alliance for the Mentally Ill (AMI), mainly composed of the families of the mentally ill, became a strong voice for the chronically mentally ill. Interestingly, their major funding source was the pharmaceutical companies. So, all the stars aligned to move the mental health system away from a SDOH community mental health perspective and towards a biological perspective. And, there has been no turning back.
The widespread endorsement of SDOH by public health may be a chance to bring the pendulum back a bit and to start addressing alternative ways of understanding emotional well being and other ways of intervening and preventing disorders.
If we all embraced a SDOH perspective on mental health, what would that look like?
First, researchers would have to lay the ground work by gathering the studies
on each of the social determinants of health and its relationship to mental health. For example: What is the impact on unemployment or underemployment to one’s emotional well being? How does nutrition and fitness affect one’s mental health?
In the arena of health, an early British publication entitled “ The Solid Facts”
http://www.euro.who.int/__data/assets/pdf_file/0005/98438/e81384.pdf laid out the research to back up each social determinant of health in a clear and concise manner – very readable for stakeholders and policy makers. This is what is needed now for SDOH and mental health.
Second, for each SDOH we would need to present approaches that can modify these social determinants in such a way that it can improve the mental health of the population. These can be programs, policies or structural changes. Two recent issues that touch on major social determinants of health come to mind: At the moment there is a significant amount of focus on Food and Fitness policy . What has been found about improving food and fitness and its impact on mental health? Another hot issue at the moment regards housing; we could look at various foreclosure interventions and their impact on mental health.
So, we need a sophisticated look at how to create changes in each social determinant of health that can improve mental well being.
Finally, we need settings which can address mental health from a SDOH perspective.
Where can this work be carried out and supported? Who will step up to the plate? Mental Health agencies? Public Health agencies? Academia? Healthy Community initiatives? Or, will we need to create new settings. Without settings to support SDOH and mental health, we will make little progress.
A story that summarizes the issue well:
Early in my career, I went to do a focus group with some community elders. I asked them “What are the major issues they face in their lives?” They responded: money (not enough), access to affordable health care, and lack of transportation. Then, I explained that I was from a mental health agency and asked what issues in their life most affected their mental health. They said : ‘Doc weren’t you listening : money (not enough), access to affordable health care, and lack of transportation.’
Even back then, they understood the relationship of SDOH to their mental well being. Now, we need to catch up with them.
1 comment so farManaging competition and turf in coalitions: Ask Dr. Coalition November 15, 2011
Posted by tomwolff in : Coalition Building, Collaborative Solutions, Uncategorized , add a commentDear Dr. Coalition,
In my local coalition all the organizational members talk about working for the good of the community. But in reality they are driven by their own self interest. They spend much of their coalition time protecting their territory. Turf wars seem to dominate.
So we really don’t identify what the community needs and coordinate our resources for the good of the community
Any ideas?
Frustrated by turf wars in Illinois
Dear Frustrated,
A clear and explicit goal of coalitions is often to promote coordination, cooperation and collaboration. – to do together that which we cannot do apart. But it comes as no surprise that turf, territoriality and competition among coalition members is a major barrier to coalition success. The capacity of one organization to feel competitive with another often amazes me.
This competition can be just among health and human service agencies as the compete for clients and contracts , but it also can be between private sector and public sector, between local government and state government, or between local government and the community. A new request to provide a service might be issued by the state and two or three different agencies – all members of the same coalition- might begin to compete for that contract, seemingly undermining the coalition’s goal of cooperation.
One would hope that having declared themselves wanting to be part of a coalition, these turf battles would decline – but instead they often escalate.
So what can we do?
A good clear first step is to create a common vision (see The Power of Collaborative Solutions for an easy visioning exercise). This will set up your common goal for all to see.
Then identify (brainstorm) the steps that are needed to reach the vision. This will set out some doable steps that you can take together.
Use priority dots to pick your starting point. Next you are off and running in a direction to meet the community’s needs and hopefully reduce the turf issues.
Here is the bottom line: I know it may sound like heresy to say this, but we need to get competition out of the helping system; it seems to cause much more harm than good. Competition and helping do not necessarily go well together. We need to replace competition with cooperation and collaboration.
Dr Coalition
Dear Reader: What would you suggest to Frustrated in Illinois?
And what coalition dilemmas are you struggling with?
Please comment below:
Add a commentHelp I am trapped in a Coalition and can’t get out: Meet Dr.Coalition September 26, 2011
Posted by tomwolff in : Coalition Building, Collaborative Solutions , add a commentSo let’s ask Dr Coalition about what traps us in coalitions where there is a failure to act and what we can do to turn that around.
Dear Dr. Coalition,
I am in a coalition that talks, talks, talks but never acts. This failure to act makes me feel trapped. The members of our coalition can talk about issues endlessly. If anyone suggests taking action they urge them to first do a careful needs assessment, even though we have shelves of these assessments already. It is almost as if they don’t know how to take action or are afraid of taking any action. What can we do?
Sincerely,
Exasperated in Ohio
Dear Exasperated,
I’ve seen it all as well– coalitions are creative in finding ways to put off being catalysts for community change and moving to action to change programs, policies and practices in their communities. I have seen coalitions:
- Spend a year writing by-laws and incorporating (to what end?
- Conduct another round of needs assessments when they already have all the data they need
- Write reports summarizing their findings – reports that get placed on the shelf next to earlier reports but no one plans actions to follow up on the identified needs
- Spend all their time networking and exchanging information with each other without ever moving to the next levels of collaborative functioning – coordinating, cooperating and collaborating – these later three can create actions that move towards actual community change
So how do we get stuck coalitions to move to action? Here are some ideas:
First, identify that the lack of action is a problem that many members are experiencing (just ask them!). The literature on successful coalitions says that one of the key variables in successful coalitions is that “outcomes matter”. So tap into that sentiment among your members – that they joined the coalition and continue to commit time to it in order to create community change.
Then together identify some “low hanging fruit” – easy win situations where they can start to act together – they need to see that the core premise of coalitions will work for them – namely “That they can do together that which that they cannot do apart”. They won’t believe that until they act together and get something done.
One helpful tool is “The Continuum of Collaboration Worksheet”. This allows a coalition to assess whether they are mainly doing “networking” which does not involve taking action or whether they have moved on to other more powerful forms of coalition action – namely “coordination” “cooperation” or “collaboration”. This tool, based on Arthur Himmelman’s definitions, is available in The Power of Collaborative Solutions p. 52 ( https://www.tomwolff.com/healthy-communities-tools-and-resources.html) and also on my website (https://www.tomwolff.com/collaborative-solutions-newsletter-summer-05.htm#resources).
In future blogs Doctor Coalition will tackle other common coalition issues, such as:
- Lack of a common vision
- Failure to provide and create collaborative leadership
- Costs outweigh the benefits
- Minimal organizational structure
- Turf and Competition
- Bad history
- Not engaging self-interest
- Over-coalitioned communities
Please send Doctor Coalition the coalition dilemmas and issues that you are struggling with.
Comment on your ideas on how to address failure to act or pose your own dilemma below.
Add a commentNew Hospital Community Benefit Requirements: Who Will They Benefit? August 22, 2011
Posted by tomwolff in : Uncategorized , 1 comment so farI was recently invited to present at a Centers for Disease Control and Prevention (CDC) meeting in Atlanta regarding new requirements in the recently passed Affordable Health Care Act and also in new IRS regulations concerning Hospital Community Benefits.
Yes, the IRS is regulating hospital community benefits!
Sounds boring? Think again. This is a real opportunity for communities to partner with local hospitals on key community issues.
What are Community Benefits? Non profit hospitals earn their non-profit status by demonstrating that they have met community health needs that have been determined by a community health needs assessment. This can be a meaningful community collaboration process or it can be window dressing. So, new regulations by HHS and the IRS are trying to ensure that the process has meaning.
A number of years back I was involved in a process of voluntary community benefit guidelines for hospitals and HMOs being piloted by then Massachusetts Attorney General Scott Harshbarger. Through the trials and tribulations of that process we all learned many lessons that can be brought to bear on this present effort. My role, as the founder of Healthy Communities Massachusetts, in this earlier process was to organize the community side of the equation – local groups that mobilized to hold their community hospitals accountable.
What we discovered was that a few hospitals took the community benefits process seriously and did a great job of partnering with their local communities and developing effective, responsive and relevant community programs. However, most hospitals tried to do the minimum. Their Community Benefits Committees did not represent those most affected by the issues from the grassroots in their community but rather represented the “usual suspects” like local community non-profits, many of whom already held contracts with the hospital.
It was a major effort just to get many of the hospitals to submit their annual reports that described their required community assessments and their community benefit activities in the community. Most fascinating was that when we looked at the reports in many cases we saw almost no correlation between the community assessments and what the hospitals actually did. Their community needs assessment process may have determined that their community need was X and yet they provided Y because Y was more in tune with their mission and plan. Clearly this voluntary process needed more bite to be effective.
So fast forward to 2011, and we see potentially much the same scenario. At this excellent conference, we heard of outstanding examples of hospitals doing a great job of community benefits. I think of the work of Dory Escobar at St Joseph’s Health System in Sonoma County California. Dory is the Director of Healthy Communities and is a community organizer and her work represents those values. Her organizational framework has three areas: Advocacy Initiatives, Healthy Communities Programs and Community Health Programs. (See www.stjosephhealth.org).
We also heard of valuable tools from Julie Willems Van Dijk (U.Wisconsin) like a county system of health rankings. The Rankings are based on a model of population health that emphasizes the many factors that, if improved, can help make communities healthier places to live, learn, work and play. Building on the work of America’s Health Rankings the University of Wisconsin Population Health Institute has used this model to rank the health of Wisconsin counties every year since 2003. Rankings are now available for all counties in the country www.countyhealthranking.org.
Check it out for your county.
When I had my ten minute chance to present -(http://nnphi.org/CMSuploads/Panel%207%20-%20Wolff.pdf ) –
I urged hospitals to engage in true collaboration with those most affected by the issue in the community – with true collaboration described as relationships where we enhance the capacity of each other. I also suggested that community engagement go beyond the needs assessment stage of the process. Rather community partners need to share decision making throughout the community benefit process including setting priorities, implementation, and evaluation. I used the work of the Center for Health Equity and Social Justice at the Boston Public Health Commission as a model of this approach (see https://www.tomwolff.com/collaborative-solutions-newsletter-summer-10.htm).
So what happens from here on out?
These new regulations are an occasion for all of us to engage with our local hospitals. We must ask what they will be doing to meet these new requirements and tell them how we would like to partner with them in the process of creating their community needs assessment and then continue to work with them on the implementation of their community benefit programs that will meet the identified needs.
My good colleagues at the Community Tool Box (http://ctb.ku.edu) at the University of Kansas have been contracted by the CDC to develop “Recommended Practices for Enhancing Community Health Improvement”. This will be a very comprehensive tool kit based on the wonderful resources of the Community Tool Box for the community needs assessment process. I will try to keep you informed as to when these resources will go public.
To comment click above
1 comment so farTime to Transform our Health and Human Service System July 22, 2011
Posted by tomwolff in : Uncategorized , 2commentsThe time has come for us to rethink and transform the health and human services system in this country. These services cover a vast array of organizations providing a very broad range of services and consume large parts of federal, state and local budgets. The services are often critical for the consumers but the core premises on which the system is based and the system of delivery itself is highly dysfunctional.
The delivery system is characterized by:
1) A focus on individuals not communities and ignores the environment in which the individual lives
2) Focuses on the deficits of the individual and the community not their strengths and assets
3) Services remain targeted at crises and remedial services ignoring how prevention could prevent the problem from occurring in the first place by catching issues upstream
4) Our systems fail to respond to the diversity of our communities much less address issues of structural oppression, racism etc.
5) Our helping systems excessively rely on professionals and fail to acknowledge and engage the natural helping systems of families and neighborhoods. Increasingly our helping systems have become detached from the communities they serve.
6) Our helping system fails to engage those most affected by the issue as equal partners in planning, delivering and evaluating their interventions.
7) As a system the health and human services in any given community tends to be: competitive rather than collaborative; fragmented so that individuals are treated for distinct problems rather than as whole beings; efforts are duplicated due to lack of information rather than coordinated
8) Finally the helping system and many of those working in the system have lost their spiritual purpose. They may have chosen their fields with hopes of addressing the common good and now end up counting billable hours.
These system dysfunctions are discussed at greater length in my book The Power of Collaborative Solutions www.tomwolff.com
I have been preaching these dysfunctions and their solutions for decades so it was a delight to find a fellow traveler and another community psychologist on this campaign in Isaac Prilleltensky , the Dean of the School of Education at the University of Miami.
Isaac contrasts systems that he describes as SPEC vs DRAIN with SPEC systems standing for systems based on Strength, Prevention, Empowering and Community. While DRAIN stands for Deficit, Reactive, Arrogant, Individual.
More details on Isaac’s system are available at their web site: http://www.specway.org/wiki/collaboration
Many of us have some stories of individual systems, agencies or interventions that have been able to move from SPEC vs DRAIN (see community stories in my book, or previous issues of my Collaborative Solutions Newsletters www.tomwolff.com ). These stories need more public airing.
However, the urgent questions now facing all of us are how do we transform our dysfunctional helping system to a strength based system that addresses the system shortcomings noted above and moves in new positive directions.
The present fiscal crisis is leading to dramatic cuts of funding to this helping sector but as noted in my last newsletter (Thriving and Surviving in Hard Times) this is not leading to system transformation but rather retrenchment to a more dysfunctional system. We are cutting prevention and keeping remediation, cutting community wide healthy community programs and keeping services for individuals, etc.
I’d love to hear your thoughts on how to convert our dysfunctional helping systems to ones that are focused on communities, prevention, strengths, our community’s diversity, build on community helping systems, bring those most affected by the issues to the table as equal partners, operate collaboratively, and engage our spirituality as the compass for social change. What are your ideas for transformation of our nation’s health and human service systems.
Add your comments above
2comments